PFE vs Cortisone Injections: A New Path for Lasting Heel Pain Relief
For millions of people living with chronic heel pain from plantar fasciitis, the cortisone shot has long been a familiar, if temporary, friend. When that stabbing pain in your heel becomes unbearable — making every first step in the morning feel like walking on broken glass — a quick injection can feel like a miracle, offering weeks or even months of relief that allow you to get back to your life. But as anyone on this cycle knows, the relief is often fleeting. The pain inevitably returns, and you find yourself back in the doctor’s office, counting down the months until your next shot. This repetitive cycle can be frustrating, and with each injection, the benefits can diminish while the risks grow.
What if there was a way to break this cycle? What if, instead of just masking the inflammation, you could address its underlying source? This is the promise of an advanced, minimally invasive treatment called plantar fasciitis embolization (PFE). PFE is not another injection; it is a targeted procedure that reduces the abnormal blood flow feeding the inflammation in your plantar fascia, offering the potential for significant, long-lasting pain relief.
If you are tired of the cortisone injection treadmill and are seeking a durable solution that doesn’t involve major surgery, this guide is for you. We will compare the old standby — cortisone injections — with the innovative PFE procedure offered at Fox Vein & Vascular, exploring how they work, who they are for, and why PFE may represent a better path forward for managing chronic plantar fasciitis.

Understanding the Problem: Inflammation in Chronic Plantar Fasciitis
Before comparing treatments, it is essential to understand the root of the problem. Plantar fasciitis is often described as a simple overuse injury where the thick band of tissue connecting your heel bone to your toes becomes irritated and inflamed. While repetitive strain is a factor, the chronic pain associated with long-standing plantar fasciitis is driven by something deeper: a process called neovascularity.
When the plantar fascia remains inflamed for months, the body responds by growing new, abnormal blood vessels into the damaged tissue. These tiny vessels create a vicious cycle — more blood flow feeds more inflammation, which generates more pain, which triggers more abnormal blood vessel growth. This is why heel pain that has lasted six months or longer often stops responding to treatments that worked early on.
Both cortisone injections and PFE aim to break this inflammatory cycle, but they do so in fundamentally different ways. Understanding this distinction is the key to choosing the right treatment for your situation.
The Traditional Approach: Cortisone Injections
Cortisone shots have been a cornerstone of heel pain treatment for decades. Cortisone is a powerful corticosteroid, a synthetic drug that mimics cortisol — a hormone your body naturally produces to suppress inflammation.
How Do Cortisone Injections Work?
When injected directly into the area around your plantar fascia, cortisone acts as a potent anti-inflammatory agent. It works by:
- Suppressing inflammatory cells: It calms the overactive immune cells that are releasing inflammatory chemicals in and around your plantar fascia.
- Reducing swelling: By tamping down the inflammatory response, the injection helps reduce swelling and irritation at the heel.
- Blocking pain signals: Less inflammation means fewer pain signals are sent to the brain, giving you welcome relief.
The procedure is quick, performed in an office setting, and can provide rapid relief — often within a few days.
The Limitations of Cortisone: A Short-Term Solution
While effective for quick relief, the primary drawback of cortisone is its temporary nature. It treats the symptoms of inflammation but does nothing to address the underlying cause — the abnormal blood vessels that are fueling the fire.
Key limitations:
- Diminishing returns: The first shot may provide months of relief, but subsequent injections often become less effective, and their duration of relief shortens over time.
- Limited frequency: Due to potential side effects, doctors typically limit cortisone injections to no more than three or four times per year in a single area.
- Risk of fascia weakening and rupture: Repeated cortisone injections can weaken the plantar fascia itself, increasing the risk of a partial or complete tear — a serious complication that can dramatically worsen your condition.
- Fat pad atrophy: Repeated steroid injections near the heel can thin the fatty cushion on the bottom of your foot, leaving you with less natural shock absorption and potentially more pain in the long run.
- Masking the problem: Because the pain relief is temporary, the underlying inflammation continues while you are feeling better, potentially allowing the condition to worsen.
For many patients, cortisone shots become a bridge to nowhere — offering just enough relief to get by but ultimately leading to the same frustrating destination: the point where conservative treatments are no longer enough.

The Advanced Approach: Plantar Fasciitis Embolization (PFE)
Plantar fasciitis embolization represents a new frontier in chronic heel pain treatment. Instead of injecting a drug to temporarily suppress inflammation, PFE targets the problem at its source — the abnormal blood supply feeding inflamed tissue. It is performed not by a podiatrist or orthopedic surgeon, but by a board-certified vascular surgeon like Dr. David Fox, MD, FACS, RPVI, who specializes in image-guided vascular interventions.
How Does the PFE Procedure Work?
The PFE procedure is a sophisticated, minimally invasive technique that selectively blocks the arteries feeding the inflammation in your plantar fascia.
Access
The procedure begins with a tiny, pinhole-sized puncture — typically at the ankle or top of the foot. Through this access point, a thin, flexible tube called a catheter is inserted into the arterial system.
Mapping
Using advanced, real-time X-ray imaging (fluoroscopy), Dr. Fox navigates the catheter to the arteries supplying the plantar fascia. He creates a detailed map of the blood vessels to identify the specific branches feeding the inflamed tissue.
Embolization
Once the target vessels are identified, microscopic embolic particles are precisely released through the catheter. These particles flow into the abnormal arteries and block them, cutting off the excessive blood supply.
Completion
Starved of its fuel source, the inflammation subsides, and with it, the pain. The catheter is removed, and a small bandage is placed over the puncture site.
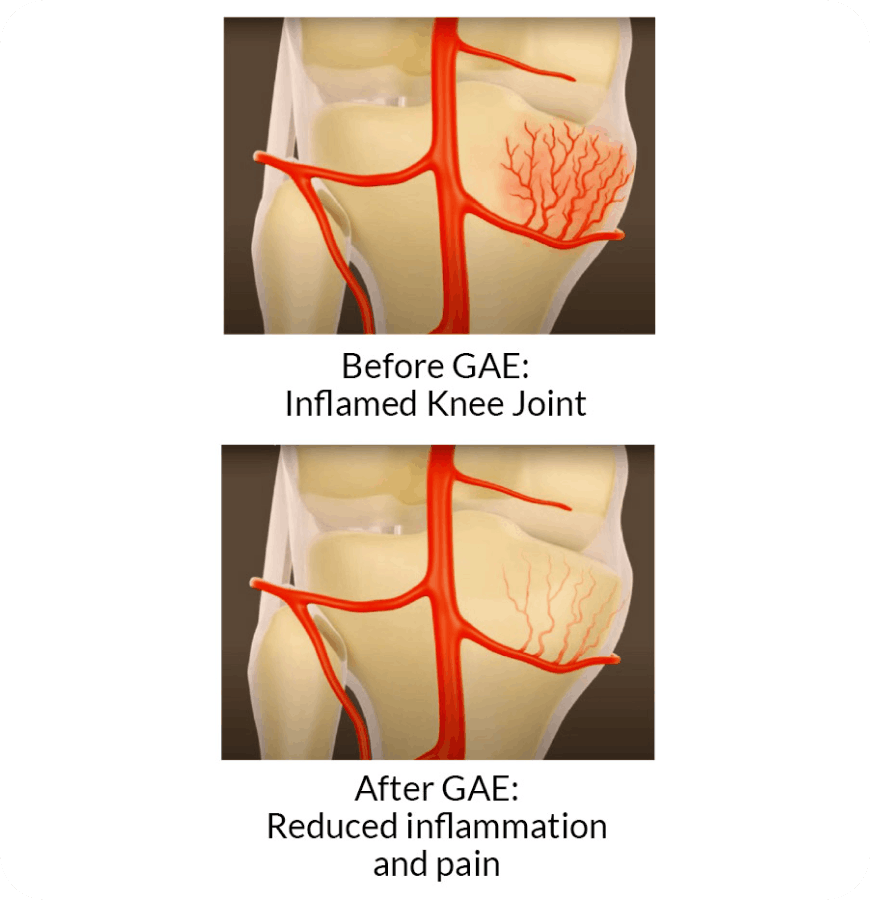
The entire outpatient procedure takes about 45 to 90 minutes, and patients go home the same day. This is the same proven embolization technology used in genicular artery embolization (GAE) for chronic knee osteoarthritis — now applied to the plantar fascia.
The Benefits of PFE: A Long-Term Strategy
The fundamental advantage of PFE is its durability. By addressing the vascular engine of inflammation, it offers the potential for significant, sustained pain relief.
Key benefits of PFE:
- Long-lasting relief: Clinical studies show that 80 to 90 percent of patients experience significant pain reduction, with meaningful improvement typically seen by two to three months after the procedure.
- Treats the source: PFE reduces the underlying abnormal blood flow rather than just masking the symptoms of inflammation.
- No fascia-weakening risk: Unlike cortisone, PFE carries no risk of weakening or rupturing the plantar fascia, and no risk of fat pad atrophy.
- One procedure vs. repeated injections: Rather than returning every few months for another shot, PFE is designed to deliver lasting results from a single treatment.
- Minimally invasive: There are no incisions, no stitches, and no general anesthesia required. Only local anesthesia is needed, with light sedation available if desired. Recovery is measured in days, not weeks.
You can learn more about how plantar fasciitis embolization works in our detailed procedure guide.
Side-by-Side Comparison
To make an informed decision, it helps to see the treatments side by side.
| Feature | Cortisone Injections | Plantar Fasciitis Embolization (PFE) |
|---|---|---|
| Mechanism | Injects anti-inflammatory drug | Blocks blood flow to inflamed tissue |
| Target | Treats the symptom (inflammation) | Treats the source (abnormal blood vessels) |
| Procedure Time | 5–10 minutes | 45–90 minutes |
| Anesthesia | Local anesthetic at injection site | Local anesthetic with optional light sedation |
| Recovery | Minimal, but potential pain flare-up | Return to light activity in 24–48 hours |
| Number of Treatments | Limited to 3–4 per year; repeated indefinitely | Typically one procedure |
| Duration of Relief | Weeks to a few months | Gradual relief over 2–6 weeks; significant improvement by 2–3 months |
| Risks | Fascia weakening/rupture, fat pad atrophy, diminishing returns | Minimal; temporary soreness at puncture site |
| Cost Over Time | Lower per visit, but adds up with repeated treatments | One-time investment for lasting relief |
| Ideal Candidate | Needs rapid, short-term relief | Seeking a durable, long-term solution after conservative treatments have failed |
Can You Have Both?
Yes — cortisone injections and PFE are not mutually exclusive. In fact, they can work together as part of a comprehensive treatment plan. If you are currently relying on cortisone to manage your heel pain, you don’t necessarily have to stop while exploring PFE.
A cortisone injection can provide valuable bridge relief — reducing your pain in the short term while the effects of PFE develop over the following weeks. Since PFE results are gradual, with most patients noticing significant improvement by two to three months, a cortisone shot can help you stay comfortable during that transition period.
Dr. Fox will evaluate your specific situation and advise on the best approach. During your consultation, he will review your imaging, discuss your injection history, and create a treatment plan tailored to your needs and timeline.
Choosing between cortisone injections and PFE depends on your goals, your treatment history, and how long you have been dealing with heel pain.
- Early-stage plantar fasciitis: If you’ve only been dealing with heel pain for a short time and haven’t yet tried conservative treatments like physical therapy, orthotics, or stretching.
- Acute flare-ups: You need rapid, short-term relief to function or get through a specific event.
- First-line treatment: Your podiatrist has recommended an initial injection as part of a broader conservative care plan.
When PFE May Be the Better Path
PFE is designed for patients with chronic plantar fasciitis who are looking for a more lasting solution. You are likely a strong candidate for PFE if:
You are on the cortisone treadmill: You have had multiple injections, and they are no longer working as well as they used to.
Conservative treatments have failed: Physical therapy, orthotics, shockwave therapy, and injections have not provided lasting relief — and your heel pain has persisted for six months or longer.
You want to avoid surgery: PFE is an ideal alternative for patients who want to avoid plantar fascia release surgery but need something more effective than repeated injections.
Pain limits your life: Your chronic heel pain prevents you from exercising, standing comfortably, or enjoying daily activities.
A consultation with Dr. Fox, including a review of your imaging and a discussion of your treatment history, is the definitive way to determine if PFE is right for you.
Schedule Your Consultation
If you’re ready to explore whether plantar fasciitis embolization is right for you, contact Fox Vein & Vascular to schedule a consultation with Dr. Fox.
Dr. Fox and his team will review your imaging, discuss your treatment history, and help you understand whether PFE could be the right next step. With more than 28 years of experience as a board-certified vascular surgeon, Dr. Fox brings the expertise and precision needed to help you move beyond temporary fixes and toward lasting heel pain relief.
Schedule a Consultation
We’re here to help you take the next step with confidence.